


Influenza ( 2009 H1N1 ) Vaccine Market
Influenza, 2009 H1N1 Global Market Trends
This knol presents an analysis of the global market for vaccines to treat Influenza ( 2009 H1N1 ) for the current year. It is estimated that the combined global market for seasonal influenza vaccine will increase by 15% in 2009 to $3500 million. The pandemic influenza vaccines market is estimated at $12 billion for the 1 billion doses a year current global output, half for the year 2009 and the other for next year. Operating at peak production the pharmaceutical industry can produce 90 million doses per week. WHO has given a price range of $20 to $2.5 for pandemic vaccine per dose. Addition of adjuvant and shift to cell cultures can stretch the present global production capacity to increase protection for world population. Results of clinical trial with tested 2009 H1N1 vaccines indicate that a single dose may offer protection to over 90% of the vaccinated subjects. The total global market for Influenza including 2009 H1N1 is projected to be $10.4 billion during the current winter (2009-2010) . If these projections are correct, the global vaccine market may grow from $24 billion in 2008 to $29 billion in the current year. These figures confirm the remarkable turnaround for the vaccine industry from the bleak horizon of late 1990s and upto 2003.
Table des matières
- Introduction
- I Never Get The Flu
- CDC Estimates of 2009 H1N1 Cases and Related Hospitalizations and Deaths from April-November 14, 2009, By Age Group
- Table 1 Types of Influenza Vaccines
- Cancelled Orders
- WHO
- CDC/FDA
- ECDC/EMEA
- Related Vaccine Articles
- Books and Monographs
LES AUTEURS
 Krishan Maggon
Krishan Maggon




Search only trustworthy HONcode health websites:
QR Code for smartphones and mobile devices
http://goo.gl/7fcS.qr
Short URL: goo.gl/7fcS
Publishers, corporations, educational, academic, government, foundations, organizations and readers are invited to read the following document for funding, sponsorship and commercial license opportunities.
The document explains author's policy: to provide trustworthy information, conflict of interest, marketplace and privacy and data protection issues.
Introduction
This knol analyses the vaccine market for seasonal and 2009 H1N1 influenza for the current year.
An attempt has been made to generate market research and intelligence data in realtime for the 2009 H1N1 pandemic outbreak.The Avian Influenza Pandemic in Asia served as a test case to plan for future pandemic outbreaks.
The lessons learned and recommendations made during the Avian Influenza H5N1 outbreak have been adopted by the industry to meet the unexpectedly high demand and to scale up production of vaccines.[1][2][3][4][5][6][7][8]
The lessons learned and recommendations made during the Avian Influenza H5N1 outbreak have been adopted by the industry to meet the unexpectedly high demand and to scale up production of vaccines.[1][2][3][4][5][6][7][8]
The current market for seasonal Influenza is dominated by two therapeutic categories: vaccines to protect vulnerable populations for seasonal (elderly, immunocompromised patients), Pandemic (children, pregnant women, obesity, chronic disease and immunocompromised patients) and neuraminidase inhibitor antivirals Tamiflu® (Roche) and Relenza® (Glaxo Smith Kline).[9] For the 2009 H1N1 Pandemic influenza vaccine sale projections, traditional methods and models are not suitable or reliable. In the past, these methods have failed to predict strong demand by arthritis patients for tumor necrosis factor alpha blockers and revival of the vaccine industry. [10][11][12] The vaccine industry requires forecast or projections due to long term planning, confirmed sales order and production scheduling to meet surging demand during Pandemic outbreak.[13][14][15][16][17][18]
Regulatory Requirements
All vaccines must pass safety and efficacy criteria for FDA/EMEA approval and marketing. Influenza vaccines are manufactured according to Good Manufacturing Practise to ensure quality. The current regulations for yearly approval of influenza vaccines (FDA, EMEA, WHO) are listed in Appendix A. These include testing for antibody titres, any transient adverse events like pain or swelling at injection site or any other adverse reactions. To qualify for registration, vaccines must generate sufficient antibody response in 70% of treated subjects within 2-3 weeks and not cause any serious adverse reaction.[19][20][21][22][23] It is very difficult to show superior safety or efficacy of one brand over any other brand or detect rare side effects in trials. Such a trial will involve over 5-10 million subjects, follow up over 1 year and will be very costly to manage, monitor and analyse with unpredictable outcome. These objectives can be achieved with current postmarketing surveillance or Vaccine Watch. The efficacy of current seasonal and pandemic influenza vaccines has ranged from 60-90%. Testing of drugs and vaccines in babies and pregnant women raises variety of ethical concerns about the need for testing, which must be addressed. NIAID has announced that it is testing the efficacy of 2009 H1N1 vaccines in high risk groups [24][25][26]. The strains for yearly influenza vaccines are selected and recommended. The current seasonal vaccine strains as recommended by experts of WHO/CDC are provided in Appendix B. The types of vaccines are described in Table 1. The regulatory burden adds to 70% of the current cost of vaccines. A new vaccine requires testing in over 10000 subjects and may cost over $ 1 billion for R&D and additional 400 million on the GMP manufacturing facility [10][12][27][28][29][30][31].
Data Collection and Analysis
A database of top selling human vaccines and biologic brands has been maintained since 2002. The information collected from company annual and quarterly reports, FDA/EMEA approval, medical meetings and financial press and media is included and regularly updated. In case of foreign currency, the exchange rate used by the company in its report is utilized for dollar conversion . The database has tracked most of the recently launched brands approved by the FDA and EMEA. Company reporting under strict SEC regulations is more reliable for sales of its own brands than commercial market research firm confidential and patented data collection methods. In case of co marketing by different companies for the same brand or active ingredient under different brand, the figures are added up to arrive at total sales. Brand names of the medicines are used as sales are reported for the brands, companies rarely provide breakdown of sales by active ingredient or generic name. The sales estimate for seasonal influenza vaccines is based on actual 6 months sales in 2009, company own sales projections and guidance for analysts and the normal sales increase during the winter influenza period from previous years [12][29][32][33]. The actual sales data from the major companies validate the above projections.
Vaccine sales are reported under a variety of categories. For influenza vaccines, sales are reported for all brands collectively or in case of low sales, combined with other types of vaccines. For the 2009 H1N1 vaccine estimate a variety of news sources, press releases by WHO, CDC, FDA, EMEA, medical journals and industry were used to collect information used in Tables 2-3. These sources and headlines are described and listed in Appendix C and D.[12][29][34]
I Never Get The Flu
Source: National Center for Immunization and Respiratory Diseases
Running Time: (1:01)Release Date: 12/15/2009http://www.cdc.gov/CDCTV/INever/index.html
Running Time: (1:01)Release Date: 12/15/2009http://www.cdc.gov/CDCTV/INever/index.html

CDC Video Player.
Flash Player 9 is required.
The pharmaceutical industry is facing a range of pressures, both logistically, ethically and politically. It is under pressure to meet high demand and is working round the clock to achieve this. In addition it has donated vaccine to the World Health Organisation, reduced prices for poor countries and charities. There are also Governmental requirements. The purchase prices of influenza vaccines and antivirals are dictated by Governments as bulk purchase. Under US law, for instance, industry has to give maximum discount to government purchasers. These discounts are in the range 20-30% of the market price. The market value of the vaccines produced is used with a standard 30% discount ( free samples, donation, volume discount etc. (See direct links to Industry Sites provided at the end of the article). Cell cultured vaccines are priced higher due to higher cost of production and suitability for persons allergic to egg proteins. Similarly Flu Mist is priced higher than traditional egg based vaccines. WHO and French media reports indicate that over 1 billion doses of Pandemic 2009 H1N1 vaccines were ordered by governments. Swiss media has indicated that its Government paid 93 million Swiss francs ( $90 million) for 13 million doses of pandemic vaccine
Most of the 2009 H1N1 vaccines produced passed current safety and efficacy criteria and were approved by regulatory authorities in major markets. These include vaccines with adjuvants, produced by cell culture and inactivated virus used in Pandemic FluMist. The FDA has not approved any influenza vaccine containing adjuvents in over 70 years. These vaccines have been available in Europe for the past five years. WHO has recommended the use of 2009 H1N1 Flu Mist for all including pregnant women. EMEA has not approved Flu Mist which has been marketed in US for over 7 years [35][36][37][38][39][40][41].
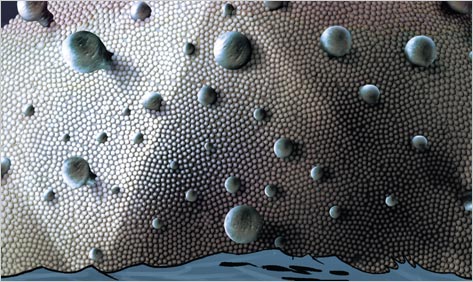
Pathogen free fertilized eggs are used. Each of the three strain of the virus is grown separately by injection and stimulating the production of antivirus antibodies. After incubation for few days, the virus is separated from egg, purified and inactivated and combined with two other starins to produce 1 dose of the trivalent seasonal influenza vaccine. The egg derived vaccine is not recommended for persons allergic to egg proteins. Flu Mist uses a live inactivated virus and is contraindicated during pregnancy and in patients with asthma and other respiratory problems in the US.

CDC PHIL ID 10759
One egg is required to produce 1 dose (15 mcg) of trivalent seasonal influenza vaccine. In case of a monovalent 2009 H1N1 Pandemic vaccine and with adjuvant, one egg may produce 2 doses or more. In case of low yields, 2 eggs may be required to produce 1 dose of vaccine. During bird flu epidemic, CDC provided $2 billion of R&D funding to the leading vaccine companies to develop cell cultured manufacture of vaccines in 2005. Cell cultured vaccines and vaccines with adjuvants are approved in Europe but not in US.
Novartis has produced pandemic H1N1 virus by cell culture using dog kidney cell line. Its cell cultured H5N1 Pandemic bird flu vaccine was approved by the EMEA but not by the FDA. Novartis has reported only 30% yield with the H1N1 pandemic vaccine as the virus grows poorly in eggs (Appendix D).
Over 90% of the current Influenza vaccines are produced in eggs and only 10% in cell cultures. Under Pandemic outbreaks, it is easier to scale up cell culture vaccine production to meet high demand.
Acambis has developed a universal influenza vaccine and has tested in Phase I trials. A monoclonal antibody for prophylalaxis is in development besides newer cell cultured and adjuvent enhanced vaccines.
Results
The list of currently approved vaccines is described in Appendix E. Appendix F lists the variety of influenza vaccines produced by Novartis in traditional egg culture, cell culture in protein free medium and with and without adjuvant MF059 and preservative thimoseral.
The sales of seasonal Influenza vaccines for the past few years is shown in Fig 1 [12][29]. There has been constant increase in the demand and use of influenza vaccine mainly in the Western World. However the coverage is still low and it does not reach all the elderly persons and children requiring protection.
Table 2 lists orders for the 2009 H1N1 vaccines placed by selected OECD Governments. Although it is the same threat, the announcements have either given the dollar amounts or doses ordered and rarely the doses and cost are listed together (USA $2 billion, France 80 million doses and over $ 1 billion, UK 60 million doses, Germany, Italy, Japan, Spain) . Sanofi Aventis and Glaxo Smith Kline have donated 100 and 50 million doses of vaccines to the WHO for distribution in poor countries. These donations amounted to 10% of production capacity of the two companies. Sanofi Aventis capacity is thus 1 billion doses and Glaxo Smith Kline 500 million doses, together the two companies account for 50% of the global production. Eight of the OECD rich countries have donated a total of 50 million doses ( Appendix C ) [33][34][36]. Sanofi Aventis is committed to supply 75 million doses of its pandemic vaccine to the US government and has increased production capacity to 125 million doses in its US plant and will supply 45% of US orders.
The 2009 H1N1 Vaccine can be sold at around $10-20 in OECD countries, in the range of $5-10 in mid level developing economies and in the range of $2.5-5 in the poor countries (paid by charities, foundations and global agencies, World Bank). This model by charging patients and countries by their ability to pay is better than providing free treatments.
Rich nations have locked in and ordered most of the current capacity for antivirals and pandemic flu vaccines. France and UK have ordered supplies to cover entire population while Germany for 30% and USA for over 40% of its population in the first phase and 80% in the second phase if required.
The CDC Revised estimates provides a good overview of the spread of the 2009 H1N1 in the US.
CDC Estimates of 2009 H1N1 Cases and Related Hospitalizations and Deaths from April-November 14, 2009, By Age Group
| 2009 H1N1 | Mid-Level Range* | Estimated Range * |
| Cases | | |
| 0-17 years | ~16 million | ~12 million to ~23 million |
| 18-64 years | ~27 million | ~19 million to ~38 million |
| 65 years and older | ~4 million | ~3 million to ~6 million |
| Cases Total | ~47 million | ~34 million to ~67 million |
| Hospitalizations | ||
| 0-17 years | ~71,000 | ~51,000 to ~101,000 |
| 18-64 years | ~121,000 | ~87,000 to ~172,000 |
| 65 years and older | ~21,000 | ~15,000 to ~29,000 |
| Hospitalizations Total | ~213,000 | ~154,000 to ~303,000 |
| Deaths | ||
| 0-17 years | ~1,090 | ~790 to ~1,550 |
| 18-64 years | ~7,450 | ~5,360 to ~10,570 |
| 65 years and older | ~1,280 | ~920 to ~1,810 |
| Deaths Total | ~9,820 | ~7,070 to ~13,930 |
* Deaths have been rounded to the nearest ten. Hospitalizations have been rounded to the nearest thousand and cases have been rounded to the nearest million. Exact numbers also are available.
Table 1 Types of Influenza Vaccines
- Seasonal Influenza Vaccines: egg based
With and without thimerosal (Multidoses contain the preservative,
single dose vials are free from it)
With and without adjuvants- FluMist Live Inactivated Virus
- Cell Cultured Seasonal Influenza Vaccines: free from egg proteins
With and without adjuvants
- 2009 H1N1 Influenza Vaccines Egg based
- 2009 H1N1 Flu Mist , Live attenuated
- Cell Cultured 2009 H1N1 Vaccines
With and without thimerosal
With and without adjuvants
Table 2. Pandemic Influenza (2009 H1N1) Vaccine Orders
| Country | Doses Ordered million | Market Value $ million |
| USA | 251 | 3750 |
| UK | 132 | 1980 |
| France | 94 | 1500 |
| China* | 65 | 650 |
| Japan | 53 | 840 |
| Germany | 50 | 900 |
| Canada | 50 | 800 |
| Italy | 48 | 765 |
| Spain | 37 | 590 |
| Netherlands | 34 | 540 |
| Portugal | 28 | 440 |
| Greece | 24 | 380 |
| Australia | 21 | 340 |
| Hungary | 20 | 320 |
| Sweden | 18 | 290 |
| Switzerland, South Korea | 13 , 13 | 210, 210 |
| Belgium | 12 | 190 |
About 1 billion doses of vaccines were ordered by governments of major economies and Western countries.


OECD countries account for 99% orders for the current world influenza vaccine production capacity.
US, UK, France, Italy, Switzerland, Australia, Brazil, Norway have annonced donation of 10% of H1N1 Vaccine to WHO for poor countries.
* Local Chinese vaccine is cheaper and costs $5-10 per dose.
How to estimate the market for Pandemic Inflenza H1N1 Vaccine, which is sold out even before production and there is limited supply insufficient to meet demand. Indirect methods have been used and data compiled from News Sources ( Appendix C, D. Table 3 )
Cancelled Orders
European Governments which ordered 2 doses per person to cover the entire population have started negotiating with the vaccine industry to cancel orders of undelivered vaccines for the 1Q 2010. France has cancelled 50 million doses of the vaccine from Sanofi Aventis, Glaxo Smith Kline and Novartis. Germany has cancelled 30% of its 50 million dose order. Greece has cancelled 75% of its order while Belgium and Norway have cancelled 30% of the order. Spain, UK, Switzerland have cancelled orders. US has cancelled orders. These cancelled orders will affect the sales in 2010 and have only minimal impact on the 4Q2009 sales of vaccines. Glaxo Smith Kline have provided an estimate of its pandemic vaccine sales in the 4Q09 as 1.36 billion dollars (130 million doses sold, 60 million donated to the WHO)
Table 3. Pandemic Influenza ( 2009 H1N1 ) Vaccine Market Forecast
WHO Production Capacity Estimate 2-4 billion doses ( 90 million doses per week maximum)
WHO Price range per dose $ 20 - $ 2.5
Donation to WHO Sanofi Aventis 100 million doses
Glaxo Smith Kline 50 million
8 Rich countries 50 million
Reduced pricing for poor countries 150 million
Produced in low cost countries 150 million
Market Price of 1 billion doses $ 15 billion
Price paid by Governments $5-8 billion
Market Price of 1 billion doses $ 15 billion
Price paid by Governments $5-8 billion
Global Market conservative estimate and WHO pricing: $ 10 billion
Market Projections for the year 2009 Influenza season : $ 5 billion
Market Projections for the year 2010 Influenza season : $ 5 billion
WHO has requested 1.5 billion dollars from donor countries to buy vaccines, Tamiflu ( $520 million) and Relenza for poor countries.
WHO has regularly increased its global vaccine production capacity estimate from 900 million, 2 billion and now 4.9 billion doses by 36 vaccine companies. Over 90% of influenza vaccine is produced in OECD countries and poor countries with population of 2.6 billion have no local vaccine production. Global syringe production is only 40 million pieces per year.
The above estimate is backed up by last year sales of seasonal influenza vaccines where
450 million doses were sold for $3.1 billion ($10 per dose). Pandemic influenza vaccine average market price is $10 per dose. News sources show large deviations, Australian government paid only $89 million for 21 million doses to CSL. Sanofi Aventis indicated a price near 7 Euro per dose (real price) for French Government, while the Government claims that it ordered 94 million doses worth 871 million euro or $1236 million (market price).[30][31][33][34]. The French government ordered 50 million doses from Glaxo Smith Kline, 28 million doses from Sanofi Pasteur, 16 million doses from Novartis at average price of 6.25 euro per dose. Baxter cell cultured Pandemic flu vaccine which can be used in persons allergic to egg proteins was purchased at a price of 10 euro per dose and the government ordered 50000 doses. German government has been criticized for paying $900 million for 50 million doses from GSK. GSK states that 22 Governments have ordered 440 million doses of its Pandemic 2009 H1N1 vaccine.
Table 4 lists the sales projections for influenza vaccines for the leading vaccine companies and Table 5 provides an estimation of the overall global influenza market.
Table 4. Pandemic Influenza ( 2009 H1N1 ) Vaccine Sales
| Company | 2009 sales $ millions |
| Sanofi Aventis | 1000 |
| Glaxo Smith Kline | 1000 |
| Novartis | 1000 |
| Baxter | 500 |
| MedImmune | 500 |
| Sino Vac | 200 |
| CSL | 200 |
| Solvay | 100 |
| Other Companies | 1200 |
| Total | 5700 |
Company sales data available, pricing and government orders are considered business secrets. Many leading companies have provided 4Q 2009 sales data. Similar levels of sales are expected in the 1Q 2010 as well by Novartis, Glaxo and Sanofi Aventis.
Assumptions:
- All the Pandemic vaccines produced by cell cultures (10%), egg based (90%), with adjuvants and pandemic Flu Mist are safe, effective and approved in the USA, Europe and Japan.
- The average price of 1 dose is $15 or Euro 10, price paid by governments are in $7-10 per dose.
- These vaccines are added to the Western Government stockpile as well.
- 10% of the production is donated to WHO or offered at reduced prices to the poor countries.
- Delay in regulatory approval, peak production level, external factors may shift >30% of the revenue to next year.
- Vaccine companies have accepted orders based on the production capacity and schedule and delivered on the first come first served basis.
Table 5 Global Influenza Market 2009
| Product | Estimated Sales 2009 $ million |
| Relenza® | 1100 |
| Tamiflu® | 3100 |
| Seasonal Vaccine | 3500 |
| Pandemic 2009 H1N1 Vaccine | 5700 |
| Total | 13400 |
If the costs of Face Mask, Hand wash soaps and antiseptic hand lotions, hospitalizations, syrups, pharmacy and doctors fees are included, the total 2009 H1N1 market was over $ 100 billion in 2009.






Talk about organic content!
Click here to try Google's latest
tool on the topic of Swine Flu.
Very COOL timeline, too.

Discussion
The leading influenza vaccine companies are Sanofi Aventis, Glaxo Smith Kline, Baxter, Novartis and Astra Zeneca (MedImmune). Two other vaccine majors Wyeth and Merck are not directly involved with the manufacture of influenza vaccines. Merck joint venture with Sanofi Aventis under Sanofi Aventis Pasteur MSD provides some sales of influenza vaccines [12][29][32]. The importance of vaccine is underlined by recent takeovers of Wyeth by Pfizer, MedImmune by Astra Zeneca and equity stake in Crucell by Johnson & Johnson.
Several other companies manufacture influenza vaccines by the traditional egg culture method. These are Solvay, Crucell, Serum Institute, SinoVac. Baxter pandemic (avian and 2009 H1N1) and Novartis seasonal influenza vaccines produced by cell cultures were approved by the EMEA in Europe. The adjuvents containing seasonal and pandemic vaccines from Glaxo Smith Kline and Novartis were approved in Europe and no safety issues emerged after several years of marketing.
Several other companies manufacture influenza vaccines by the traditional egg culture method. These are Solvay, Crucell, Serum Institute, SinoVac. Baxter pandemic (avian and 2009 H1N1) and Novartis seasonal influenza vaccines produced by cell cultures were approved by the EMEA in Europe. The adjuvents containing seasonal and pandemic vaccines from Glaxo Smith Kline and Novartis were approved in Europe and no safety issues emerged after several years of marketing.
The total global sale of seasonal influenza vaccines in 2008 were $3.0 billion. The total global market for vaccines in 2008 was $ 25 billion[12][29]. The leading influenza company was Sanofi Aventis (FluZone®) with sales of $1.08 billion followed by Glaxo Smith Kline flu vaccines (Fluarix®, Flu Laval®, Flu pandemic brands) at $520 million in 2008. The price of the leading brand FluZone was $10-13 per unit dose in the USA and Europe. However if discounts are considered, vaccine makers may only get $8-10 per dose at wholesale price. These prices are better than the 2-3 dollar per unit prices which were charged in the 1990s. Sanofi Aventis sales included supplies of pandemic avian influenza vaccine worth $300 million for stockpile in the USA. Based on 45% share of the world influenza vaccine market for Sanofi Aventis gives a figure of only $2.3 billion for the global market, which is based on IMS data. IMS has historically undervalued the vaccine and biologics market. It may not include sales by Indian, Chinese, Russian, Brazilian and South African companies. Authors estimate is backed by a recent paper from Datamonitor staff in Nature which estimated the 2008 influenza market at $ 2.8 billion.[42]. In their latest 3 Q 2009 report, Glaxo Smith Kline ($1.5 billion), Sanofi Aventis ($1 billion) and Novartis ( $750 million) have indicated expected 4Q 2009 and yearly sales increase due to Pandemic influenza vaccine.These companies have projections of similar high level of sales in the first Q of 2010 as well [43][44][45][46] . Sanofi Aventis estimates the global vaccine market to increase to $35 billion by 2013 ($ 23 in developed countries + 12 billion in developing countries) and has invested over $2.5 billion in production facilities. Sanofi Aventis total vaccine sales in 2009 are estimated at $ 5 billion.
Adverse reactions to seasonal flu vaccine include aches, fever and sore arms. Allergy to egg proteins used for vaccine cultures in some patients leads to rare cases of hives, dizziness and breathing problems. For, as yet unknown reasons, the most serious side effect, Guillain-Barrè Syndrome, is reported in 1 out of 100,000 patients receiving vaccine or 1 out of 1 million (WHO). This condition leads to serious nerve damage and muscle weakness [58][86][90][91][92][93][97][98][99][100][102][104].
Leading vaccine companies have done clinical testing of the Influenza 2009 H1N1 Vaccines in healthy volunteers. Clinical trials were started and completed in Australia, USA, China, India and Europe. The USA government tested Sanofi Aventis and CSL vaccines in 2400 healthy subjects at 8 medical and university hospitals. Most of the hospitals and virologists and investigators are involved in testing of seasonal flu vaccine. Other companies Novartis, Glaxo, Merck, Baxter had their own clinical testing programmes to obtain FDA and EMEA approval. Novartis started and completed clinical testing of its pandemic flu vaccine in 6000 volunteers in Germany, UK and USA. Sanofi Aventis clinical testing of its vaccine was completed in Europe Presence of high level of antibody titre to Swine Flu and absence of severe adverse reaction is required for for regulatory approval. Presence of sufficient levels of antibody titres determined the single dose dose schedule for most and a 2 dose schedule for children under 10 years of age. The vaccination of pregnant women hasbeen discussed and the antibody response is similat to normal adult populations. Mothers pass on antibodies to the fetus thus protecting their babies during the first 6 months of life. The Swine Flu vaccine has been
approved in US and Europe and is available in limited numbers and production may peak by December 2009. The FDA and EMEA have approved several 2009 H1N1 vaccines with ongoing review of the data and fast tracked approval of Pandemic vaccine. There is going to be sufficient vaccine for persons who want it, there is going to be shortage if everyone wants the vaccine [70][74][80][81][82][83][84][85][87][88][89][96][97][98][102][103].
The vaccine industry has done a great job by increasing production from 450 million doses in 2008 to 3 billion doses in 2009. Governments have dictated their price to the industry which provides for some profits but excludes windfall profits. A similar capacity increase during the avian influenza outbreak failed to provide any revenue or confirmed orders for the industry. Despite excellent safety record of adjuvents in Europe, none of the adjuvent containing 2009 H1N1 vaccine has been approved in the USA. Use of adjuvents can reduce the required dose by half to one third and thus make the current supply reach more subjects. Similarly cell cultured vaccine has not been approved by the FDA. Despite the safety record of the nasal spray Flu Mist, it has not been approved in the European union countries.
The vaccine industry exodus from the USA began in late 1980 under the onslaught of vaccine foes, religious rights and back to nature groups. The vaccine industry in the 1990s was characterized by low priced vaccines with low margins and threat of class action lawsuits. The vaccines sales were seasonal and unpredictable and variable with sales of few millions. The link of children vaccine containing mercury preservative thimerosal to increasing cases of autism led to over 6000 class action and product injury lawsuits in the USA. The industry was running scared from product injury and class action lawsuits and was staring at bankruptcy. By the end of last century, the vaccine nanufacturing companies in the US went down from 25 in early 1980s to only 5 by 2004. These were Wyeth, Chiron (Novartis), Merck, Sanofi Aventis Pasteur and MedImmune (Astra Zeneca). In addition after billions of dollars investment over several decades, most of the vaccines developed for Malaria, AIDS, RSV and Contraception failed in clinical trials. Thus by the end of last century industry was facing bankruptcy from class action lawsuits. On top FDA regulatory burden was increasing and a new vaccine required testing in over 10000 subjects. Industry bail out of vaccine R&D and call for protection from class action and product injury lawsuits.These developments led to the current domination of European companies Sanofi Aventis and Glaxo Smith Kline in the global vaccine market. Glaxo Smith Kline and Baxter are back and CSL is the new company in the US market [47][48][49][50][51][52][53][54][55][56][57].
During the 1998-2005 period there were vaccine shortages in the USA at regular intervals due to FDA inspection of European plants, upgrading facilities to GMP, increased production or routine maintainence.on The US vaccine shortages due to closure of Chiron facility in the UK led the the US government recognize the starategic importance of the vaccine manufacturing in the USA.
The Vaccine Injury Act was passed in 1988 to provide compansation to victims harmed by vaccines and is funded by a tax on each dose of vaccine (0.75 $) sold in the US. Currently 16 vaccines are covered under this program including seasonal influenza vaccine, Pandemic avian influenza vaccine and 2009 H1N1 vaccines and antivirals. Under this act a government court pays compensation to persons harmed by vaccines, the awards are capped and the vaccine industry is protected. After several years of litigation and review of over 940 scientific articles, and testimony from 68 experts, the special court has sided with experts of Institute of Medicine and CDC who have discounted the link between thimerosal containing MMP vaccines and autism in children. The medical and scientific communities have carefully and thoroughly reviewed the evidence concerning the vaccine-autism theory and have found no association between vaccines, thimerosal and autism.
The market for seasonal influenza vaccine is influenced by weather, duration and severity of the influenza season, media coverage, public awareness, availability and supply of the vaccine. The demand and market for vaccine remains variable and unpredictable. The revival of the vaccine industry has been helped by the launch of newer blockbuster vaccines like Prevnar and Gardasil, R&D funding worth $.3-5 billion from NIH/CDC for development of vaccines against bioterror microbes like Anthrax and production of cell cultured vaccines. The pandemic 2009 H1N1 outbreak has helped the industry and consolidates vaccine revival. It has made influenza pandemic vaccine a year round manufacturing and marketing product. Addition of pandemic vaccine in government stockpile can help the vaccine industry during its lean times and provide steady revenue stream before the next pandemics. This market is exclusively dependent on government orders for stockpile and supply and is short term and valid only for the current epidemic.However increasing opposition to mass vaccination on religious, moral, ethical safety and fear reasons may derail the safety and efficacy backed by strong scientific and medical evidence and marketing of 300-100 million doses per year [47][48][49].
approved in US and Europe and is available in limited numbers and production may peak by December 2009. The FDA and EMEA have approved several 2009 H1N1 vaccines with ongoing review of the data and fast tracked approval of Pandemic vaccine. There is going to be sufficient vaccine for persons who want it, there is going to be shortage if everyone wants the vaccine [70][74][80][81][82][83][84][85][87][88][89][96][97][98][102][103].
The vaccine industry has done a great job by increasing production from 450 million doses in 2008 to 3 billion doses in 2009. Governments have dictated their price to the industry which provides for some profits but excludes windfall profits. A similar capacity increase during the avian influenza outbreak failed to provide any revenue or confirmed orders for the industry. Despite excellent safety record of adjuvents in Europe, none of the adjuvent containing 2009 H1N1 vaccine has been approved in the USA. Use of adjuvents can reduce the required dose by half to one third and thus make the current supply reach more subjects. Similarly cell cultured vaccine has not been approved by the FDA. Despite the safety record of the nasal spray Flu Mist, it has not been approved in the European union countries.
The vaccine industry exodus from the USA began in late 1980 under the onslaught of vaccine foes, religious rights and back to nature groups. The vaccine industry in the 1990s was characterized by low priced vaccines with low margins and threat of class action lawsuits. The vaccines sales were seasonal and unpredictable and variable with sales of few millions. The link of children vaccine containing mercury preservative thimerosal to increasing cases of autism led to over 6000 class action and product injury lawsuits in the USA. The industry was running scared from product injury and class action lawsuits and was staring at bankruptcy. By the end of last century, the vaccine nanufacturing companies in the US went down from 25 in early 1980s to only 5 by 2004. These were Wyeth, Chiron (Novartis), Merck, Sanofi Aventis Pasteur and MedImmune (Astra Zeneca). In addition after billions of dollars investment over several decades, most of the vaccines developed for Malaria, AIDS, RSV and Contraception failed in clinical trials. Thus by the end of last century industry was facing bankruptcy from class action lawsuits. On top FDA regulatory burden was increasing and a new vaccine required testing in over 10000 subjects. Industry bail out of vaccine R&D and call for protection from class action and product injury lawsuits.These developments led to the current domination of European companies Sanofi Aventis and Glaxo Smith Kline in the global vaccine market. Glaxo Smith Kline and Baxter are back and CSL is the new company in the US market [47][48][49][50][51][52][53][54][55][56][57].
During the 1998-2005 period there were vaccine shortages in the USA at regular intervals due to FDA inspection of European plants, upgrading facilities to GMP, increased production or routine maintainence.on The US vaccine shortages due to closure of Chiron facility in the UK led the the US government recognize the starategic importance of the vaccine manufacturing in the USA.
The Vaccine Injury Act was passed in 1988 to provide compansation to victims harmed by vaccines and is funded by a tax on each dose of vaccine (0.75 $) sold in the US. Currently 16 vaccines are covered under this program including seasonal influenza vaccine, Pandemic avian influenza vaccine and 2009 H1N1 vaccines and antivirals. Under this act a government court pays compensation to persons harmed by vaccines, the awards are capped and the vaccine industry is protected. After several years of litigation and review of over 940 scientific articles, and testimony from 68 experts, the special court has sided with experts of Institute of Medicine and CDC who have discounted the link between thimerosal containing MMP vaccines and autism in children. The medical and scientific communities have carefully and thoroughly reviewed the evidence concerning the vaccine-autism theory and have found no association between vaccines, thimerosal and autism.
The market for seasonal influenza vaccine is influenced by weather, duration and severity of the influenza season, media coverage, public awareness, availability and supply of the vaccine. The demand and market for vaccine remains variable and unpredictable. The revival of the vaccine industry has been helped by the launch of newer blockbuster vaccines like Prevnar and Gardasil, R&D funding worth $.3-5 billion from NIH/CDC for development of vaccines against bioterror microbes like Anthrax and production of cell cultured vaccines. The pandemic 2009 H1N1 outbreak has helped the industry and consolidates vaccine revival. It has made influenza pandemic vaccine a year round manufacturing and marketing product. Addition of pandemic vaccine in government stockpile can help the vaccine industry during its lean times and provide steady revenue stream before the next pandemics. This market is exclusively dependent on government orders for stockpile and supply and is short term and valid only for the current epidemic.However increasing opposition to mass vaccination on religious, moral, ethical safety and fear reasons may derail the safety and efficacy backed by strong scientific and medical evidence and marketing of 300-100 million doses per year [47][48][49].
The French government decision to cancel previously confirmed order of 50 million doses of vaccine from Glaxo Smith Kline (32 million), Sanofi Aventis (11 million) and Novartis ( 7 million) may negatively impact the market for 2009 H1N1 vaccine in 2010. The government may have to pay penalty as the companies have to cover the cost of production. Governments of Germany, Spain and Switzerland have similarly to try and cancel orders for undelivered vaccines. These cutbacks show a declining demand for pandemic vaccine with low mortality and low uptake of the vaccine. This leaves once again vaccine companies to pick up the cost of increased production capacity? Sanofi Aventis and Novartis were expected to have sales of 1 billion and 600 million dollars for the year 2010. There is strong demand from other countries like Ukraine, UAE and European governments have sold part of their stocks.
Pandemic H1N1 pharmacovigilance
Vaccine Recalls in the US: These recalls were due to the decline in the potency of some batches of the 2009 H1N1 vaccine during testing. The antigen may be sticking to the walls of the syringe or container. No safety issues are involved and the slight drop in antigen does not alter clinical immune response in vaccinated persons.
Sanofi Aventis Pasteur has recalled 4 batches of pediatric prefilled syringes (about 800,000 doses) as the the level of antigen was below specifications during routine antigen analysis.
Astra Zeneca (MedImmune) has recalled 4.7 million doses (13 lots) of its Nasal spray Vaccine as the potency of the vaccine was lower than the predetermined specifications during its routine testing
Status at 24 March 2010
This update by the European Medicines Agency (EMA)
WHO has reported 16800 deaths from H1N1 pandemic and the disease had spread to 213 countries and territories.
The disease killed 2840 victims in Europe.
A total of 14015 ADRs were reported, a vast majority were non serious
There were 2078 serious cases due to 2009 H1N1 infections in Europe.
The benefit/risk ratio of pandemic vaccines and antivirals remains positive and no serious adverse event has been reported so far.
About 50 million persons (544000 pregnant women) have been vaccinated in the European Union. Over 165 million doses of the vaccines were distributed
The reported adverse reactions with the 3 approved vaccines (Celvapan, Focetria and Pandemrix) have been as expected, mild and reversible
symptoms such as fever, nausea, headache, allergic reaction, injection site pain and swelling.
There were 130 cases related to abortion (57), stillbirth (11), Premature labor and baby (11) and 13 other pregnancy related outcomes. The normal rate of fofoetal mortality in EU is 2.6 to 9.1 per 1000 births and abortions/miscarriage is 12-15%. Thus the total number of cases reported with vaccines are within normal background range of the population.
There were 49 cases of Guillain Barre Syndrome and 1 case of Miller Fischer Syndrome (variant of GBS) were reported in relation to pandemic vaccines were reported to the EMEA. Considering that 42 million persons were vaccinated and these are considered normal background rates of GBS (1.1-1.8 per 100,000 persons). Multiple sclerosis 13 cases were reported, 2 on Focetria and 9 with Pandemrix. Out of 13 cases, 9 were with preexisting MS which flared up and 2 were within a short span after vaccination.
| Vaccine/Antiviral | Doses Distributed million | Persons injected/treated million | Adverse Drug reactions Reports No ADRs | Serious ADRs |
| Celvapan | 9.1 | 659000 | 518 - | 21 eye disorders |
| Focetria | 36 | 6.5 | 2947 5228 | 6 facial palsy, 6 intra uterine deaths, 4 deaths |
| Pandemrix | 112 | 29 | 10547 | 5 thrombocytopenia, 5 hearing loss, 3 seizures, 1 delayed hypersensitivity, 1 death, 26 deaths underlying causes |
| Tamiflu | 21.1 | 1058 | 2 deaths |
Background cases in General population
Fetal deaths 4-5 per 1000 deliveries
Facial palsy 29-36 per 100000
GBS Syndrome 2 per 100000
Thrombocytopenia 5-10 per 100000
Deaths
Most of the deaths reported after vaccinations were due to underlying risk factors
or chronic diseases.
High risk of hospitalizations and fatalities in children and pregnant women.
Close Monitoring Required
Eye disorders
Seizures linked to poorly controlled epilepsy
Delayed hypersensitivity reaction
Using the same methodology CDC has again updated the estimates to include the time period.
- CDC estimates that between 42 million and 86 million cases of 2009 H1N1 occurred. The mid-level in this range is about 59 million people infected with 2009 H1N1.
- CDC estimates that between about 188,000 and 389,000 H1N1-related hospitalizations occurred. The mid-level in this range is about 265,000 2009 H1N1-related hospitalizations.
- CDC estimates that between about 8,520 and 17,620 2009 H1N1-related deaths occurred. The mid-level in this range is about 12,000 2009 H1N1-related deaths.
FDA/CDC Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD).
March 24, 2010
FDA and CDC are assessing H1N1 vaccine safety on a continuing basis and have published a detailed report describing the safety profile of H1N1 vaccines in the United States (http://www.cdc.gov/mmwr/preview/mmwrhtml/mm58e1204a1.htm).
About 127 million doses of the H1N1 vaccine were shipped and 86 million persons vaccinated with 91 million doses. This report analyzes the safety data after 11.3 million doses of live, attenuated monovalent vaccine (LAMV) for intranasal administration and 34.9 million doses of monovalent, inactivated, split-virus or subunit vaccines for injection (MIV) were distributed. As noted in the report, FDA and CDC evaluated 10172 reports of adverse events submitted to VAERS.
The analysis of VSD data was based on 438,376 people vaccinated with H1N1 vaccines (323,345 MIV and 115,031 LAMV) in
managed-care organizations in the VSD as of November 24. No substantial differences between H1N1 and seasonal influenza vaccines were noted in the proportion or types of serious adverse events reported. No increase in any of the pre-selected adverse events under surveillance, such as Guillain-Barré syndrome, has been seen in VSD data. There were 6% or 553 reports of serious adverse events including 40 deaths. preliminary investigations fail to account for a common cause of deaths or linkage to vaccination. There were 56 reports of Guillian Barre Syndrome, each week, 80-160 cases of GBD are reported in US.
According to the January 22, 2010 update of FDA and CDC vaccine safety monitoring activities, as of January 15, 2010, the total number of doses of H1N1 vaccines distributed was 127 million and the vast majority (93%) of adverse events reported to VAERS were classified as "non-serious" (e.g., soreness at the vaccine injection site). Weekly updates on FDA and CDC vaccine safety monitoring activities are available through the VAERS web site (http://vaers.hhs.gov/resources/h1n1update#top).
The National Vaccine Advisory Committee (NVAC) created the H1N1 Vaccine Safety Risk Assessment Working Group to review 2009 H1N1 vaccine safety data. This working group of outside experts conducts regular, rapid reviews of available data from the federal safety monitoring systems and presents them to NVAC and federal leadership for appropriate policy action and follow-up available at (http://www.hhs.gov/nvpo/nvac/index.html).
To date, our experience with the H1N1 influenza vaccination program has met high safety expectations, based on the track record of the licensed seasonal vaccines, including live attenuated and inactivated vaccines. We are also collaborating with other agencies around the world to share our vaccine safety information and experiences. Should any safety concerns arise, we will evaluate them thoroughly and bring them to the public’s attention quickly.
VAERS Summary:
As of December 30, 2009, 99.3 million doses of 2009 H1N1 vaccine had been shipped to vaccination providers in the United States.
As of December 30, 2009, VAERS had received 7326 adverse event reports following 2009 monovalent H1N1 vaccination.
The vast majority (94%) of adverse events reported to VAERS after receiving the 2009 monovalent H1N1 vaccine are classified as “non-serious” (e.g., soreness at the vaccine injection site).
Of the 10172 reports, 636 (6%) were reports that were classified as “serious” health events (defined as life threatening or resulting in death, major disability, abnormal conditions at birth, hospitalization, or extension of an existing hospitalization)*.
The percentage of reports involving what would be considered serious health events is not different between 2009 H1N1 and seasonal influenza vaccines. Additionally, no new or unusual events or pattern of adverse events have emerged.
Among the 440 reports of serious health events, there were 51 reports of death. Preliminary findings do not indicate a common cause or pattern (such as similarities in age, gender, geographic location, illness surrounding death, or underlying medical conditions) to suggest that these deaths were associated with the vaccine.
VAERS has received 103 reports of Guillian-Barré syndrome (GBS), for which follow-up assessments are underway. In the United States, about 80-160 cases of GBS are expected to occur each week, regardless of vaccination.
VAERS Limitations
When reviewing data from VAERS, please keep in mind what the system is designed to do and what it is unable to do:
o VAERS is a national reporting system, in which reports are submitted voluntarily by people who think an adverse event occurred after vaccination. VAERS does not solicit reports in any systematic way from all people who have been vaccinated. Reports can be submitted by anyone, including healthcare providers, patients, or family members. Because of this feature, VAERS reports may and often do include incorrect and incomplete information. VAERS reports often lead to more complete follow-up and review of medical records.
o VAERS staff follow-up on all serious and other selected adverse event reports and obtain additional medical, laboratory, and/or autopsy records when available. As a result of the follow-up/review process, coding terms (e.g., serious or non-serious) for individual VAERS reports may change based on the information received. These changes are reflected in the weekly updates of VAERS data in the WONDER database. VAERS data in WONDER should be used with caution because numbers and conditions are often updated. Events reported in VAERS should not be viewed as evidence that the vaccine directly caused the event. Data does not infer causality. Further investigation is warranted.
o Underreporting, or failure to report events, is also one of the main limitations of VAERS. Serious medical events are more likely to be reported than minor events.
o Most importantly, VAERS cannot determine cause-and-effect. VAERS accepts all reports without regard to whether or not the event was caused by the vaccine. The report of an adverse event to VAERS does not mean that a vaccine caused the event. It only indicates that the event occurred sometime after administration of the vaccine. Proof that the event was caused by the vaccine is NOT required in order for VAERS to accept the report.
o No reports are deleted from VAERS. Therefore, it is possible to have more than one VAERS report on an individual case (e.g., a physician and a patient may have filed separate reports for the same case).
WHO
WHO expert panel recommends a single dose of 2009 H1N1 vaccine for all subjects including children. WHO endorses use of already approved adjuvents in pandemic vaccines and has recommended the use of nasal spray live attenuated vaccine FluMist 2009 H1N1 for pregnant women.
CDC/FDA
Although adjuvents are considered safe, the adjuvent containing pandemic vaccines were not approved in the US. Recommends 2 dose schedule for children 6 months to 9 years old. The live virus containg nasal spray FluMist is not recommended for pregnant women and children less than 2 years of age.
ECDC/EMEA
Has not approved the use of live attenuated virus containing nasal spray FluMist in Europe. Adjuvents containing vaccines (As04 and MF059) are approved. Recommends 2 dose schedule of the pandemic flu vaccine for all inspite of clinical studies showing immuno protection with one dose of vaccine. This may be a way to cover European experts and politicians who ordered 2 dose of vaccine per person?
Acknowledgement
Thanks are due to Mr. Jean-Antoine de Mandato (PDP, Geneva) for providing office facilities and administrative support.
Conflict of Interest
Author KM works in the pharmaceutical and biotechnology industry which may imply conflict of interest to readers.
Authors do not endorse any brands and companies mentioned in this article.
Enquiries about funding or sponsorships of this article are welcome.
Share and Communicate
 Social Bookmarking
Social Bookmarking Centers for Disease Control (CDC)
Centers for Disease Control (CDC)2009 H1N1 Flu
Site last updated December 28, 2:00 PM ETSituation Update
The weekly activity update is being provided one day early due to the Federal Holiday on Friday. Flu activity continued to decline in the United States during the week of December 13-19, 2009, as reported in FluView. The number of states reporting widespread flu activity decreased from 11 to 7. Visits to doctors for influenza-like illness, flu-associated hospitalizations, and flu-associated deaths all declined from the previous week. Flu is unpredictable and activity can rise and fall throughout the season, but flu is is likely to continue for months caused by either 2009 H1N1 viruses or regular seasonal flu viruses. In addition to seasonal flu vaccine, a vaccine against the 2009 H1N1 virus has been produced and is the best way to protect against the pandemic virus. Supplies of this vaccine are increasing and many places have opened up vaccination to anyone who wants it. Find a vaccine.
Flu activity continued to decline in the United States during the week of December 13-19, 2009, as reported in FluView. The number of states reporting widespread flu activity decreased from 11 to 7. Visits to doctors for influenza-like illness, flu-associated hospitalizations, and flu-associated deaths all declined from the previous week. Flu is unpredictable and activity can rise and fall throughout the season, but flu is is likely to continue for months caused by either 2009 H1N1 viruses or regular seasonal flu viruses. In addition to seasonal flu vaccine, a vaccine against the 2009 H1N1 virus has been produced and is the best way to protect against the pandemic virus. Supplies of this vaccine are increasing and many places have opened up vaccination to anyone who wants it. Find a vaccine. Other 2009 H1N1 Flu Topics
Diagnosis
How the illness is diagnosed, recommendations for lab testing…Infection Control
Healthcare guidance, occupational safety, facemasks & respirators…Antivirals/Treatment
Use of Tamiflu and Relenza for treatment or prevention of H1N1 flu…Emergency Use Authorization
Info about CDC-requested & FDA-issued EUA drugs & devices…What You Can Do to Stay Healthy
- Get vaccinated. Vaccination is the best protection we have against flu.Seasonal flu vaccine is available now and initial doses of 2009 H1N1 flu vaccine also are available, with additional doses available later this year.
- Influenza is thought to spread mainly person-to-person through coughing or sneezing of infected people.
- Take everyday actions to stay healthy.
- Cover your nose and mouth with a tissue when you cough or sneeze. Throw the tissue in the trash after you use it.
- Wash your hands often with soap and water. If soap and water are not available, use an alcohol-based hand rub.
- Avoid touching your eyes, nose and mouth. Germs spread that way.
- Stay home if you get sick. CDC recommends that you stay home from work or school and limit contact with others to keep from infecting them.
- Follow public health advice regarding school closures, avoiding crowds and other social distancing measures.
- Stay informed. This website will be updated regularly as information becomes available.
- Call 1-800-CDC-INFO for more information.


- Email page
- Print page
View page in
Get email updates
To receive weekly email updates about this site, enter your email address:What's this?Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333
- 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348
24 Hours/Every Day
- cdcinfo@cdc.gov
Add this button to your website

Spread the word
Site last updated December 28, 2:00 PM ET
Situation Update
The weekly activity update is being provided one day early due to the Federal Holiday on Friday.
Flu activity continued to decline in the United States during the week of December 13-19, 2009, as reported in FluView. The number of states reporting widespread flu activity decreased from 11 to 7. Visits to doctors for influenza-like illness, flu-associated hospitalizations, and flu-associated deaths all declined from the previous week. Flu is unpredictable and activity can rise and fall throughout the season, but flu is is likely to continue for months caused by either 2009 H1N1 viruses or regular seasonal flu viruses. In addition to seasonal flu vaccine, a vaccine against the 2009 H1N1 virus has been produced and is the best way to protect against the pandemic virus. Supplies of this vaccine are increasing and many places have opened up vaccination to anyone who wants it. Find a vaccine.Other 2009 H1N1 Flu Topics
Diagnosis
How the illness is diagnosed, recommendations for lab testing…
Infection Control
Healthcare guidance, occupational safety, facemasks & respirators…
Antivirals/Treatment
Use of Tamiflu and Relenza for treatment or prevention of H1N1 flu…
Emergency Use Authorization
Info about CDC-requested & FDA-issued EUA drugs & devices…
What You Can Do to Stay Healthy
- Get vaccinated. Vaccination is the best protection we have against flu.Seasonal flu vaccine is available now and initial doses of 2009 H1N1 flu vaccine also are available, with additional doses available later this year.
- Influenza is thought to spread mainly person-to-person through coughing or sneezing of infected people.
- Take everyday actions to stay healthy.
- Cover your nose and mouth with a tissue when you cough or sneeze. Throw the tissue in the trash after you use it.
- Wash your hands often with soap and water. If soap and water are not available, use an alcohol-based hand rub.
- Avoid touching your eyes, nose and mouth. Germs spread that way.
- Stay home if you get sick. CDC recommends that you stay home from work or school and limit contact with others to keep from infecting them.
- Follow public health advice regarding school closures, avoiding crowds and other social distancing measures.
- Stay informed. This website will be updated regularly as information becomes available.
- Call 1-800-CDC-INFO for more information.
- Email page
- Print page
View page in
Get email updates
To receive weekly email updates about this site, enter your email address:
What's this?Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348
24 Hours/Every Day - cdcinfo@cdc.gov
Add this button to your website
Spread the word
 Send an e-card
Send an e-cardSite last updated December 11, 3:00 PM ET
Dec 1 ALERT: Fraudulent emails referencing CDC-sponsored State Vaccination Program »
 During the week of November 29-December 5, 2009, flu activity continued to decline in the United States as reported in FluView. The number of states reporting widespread flu activity decreased from 25 to 14. Visits to doctors for influenza-like illness and flu-associated hospitalizations declined from the previous week, however flu-associated deaths increased.
During the week of November 29-December 5, 2009, flu activity continued to decline in the United States as reported in FluView. The number of states reporting widespread flu activity decreased from 25 to 14. Visits to doctors for influenza-like illness and flu-associated hospitalizations declined from the previous week, however flu-associated deaths increased.
See More On Key Flu Indicators »
Situation Update
During the week of November 29-December 5, 2009, flu activity continued to decline in the United States as reported in FluView. The number of states reporting widespread flu activity decreased from 25 to 14. Visits to doctors for influenza-like illness and flu-associated hospitalizations declined from the previous week, however flu-associated deaths increased. See More On Key Flu Indicators »
Other 2009 H1N1 Flu Topics
Diagnosis
How the illness is diagnosed, recommendations for lab testing…Infection Control
Healthcare guidance, occupational safety, facemasks & respirators…Antivirals/Treatment
Use of Tamiflu and Relenza for treatment or prevention of H1N1 flu…Emergency Use Authorization
Info about CDC-requested & FDA-issued EUA drugs & devices…What You Can Do to Stay Healthy
- Get vaccinated. Vaccination is the best protection we have against flu. Seasonal flu vaccine is available now and initial doses of 2009 H1N1 flu vaccine also are available, with additional doses available later this year.
- Influenza is thought to spread mainly person-to-person through coughing or sneezing of infected people.
- Take everyday actions to stay healthy.
- Cover your nose and mouth with a tissue when you cough or sneeze. Throw the tissue in the trash after you use it.
- Wash your hands often with soap and water. If soap and water are not available, use an alcohol-based hand rub.
- Avoid touching your eyes, nose and mouth. Germs spread that way.
- Stay home if you get sick. CDC recommends that you stay home from work or school and limit contact with others to keep from infecting them.
- Follow public health advice regarding school closures, avoiding crowds and other social distancing measures.
- Stay informed. This website will be updated regularly as information becomes available.
- Call 1-800-CDC-INFO for more information.
- Email page
- Print page
View page in
Get email updates
To receive daily email updates about this site, enter your email address:Enter Email Address Submit Button What's this?
Contact Us:
- Centers for Disease Control and Prevention
1600 Clifton Rd
Atlanta, GA 30333 - 800-CDC-INFO
(800-232-4636)
TTY: (888) 232-6348
24 Hours/Every Day - cdcinfo@cdc.gov
Swine Flu Info
Quick Question
Are these search results helpful to you? Why or why not?
Thank you for helping us improve our site.
Add this button to your website

Spread the word
 Send an e-card
Send an e-card
FDA 2009 H1N1 (Swine) Flu Page
The FDA plays a vital role on the team led by the U.S. Department of Health and Human Services in the fight against the 2009 H1N1 virus. The agency works closely with the Centers for Disease Control and Prevention, National Institutes of Health, other federal government agencies, and global partners such as the World Health Organization and foreign governments to protect public health during the 2009 H1N1 pandemic. Topics on this Page: |
H1N1 Flu Vaccine
FDA ensures the safety, effectiveness and supply of the H1N1 flu vaccine.- How the flu vaccine is made (PDF, 248 KB)
- H1N1 vaccine ingredients
- H1N1 vaccine questions and answers
- Use of Influenza A (H1N1) 2009 Monovalent Influenza Vaccine in Pregnant Women
- Dear health care professionals letter regarding 2009 H1N1 flu virus (June 18)
- Complete information on each H1N1 flu vaccine
- Injectable vaccine
- Intranasal vaccine
- Safety monitoring
- FDA update on the H1N1 flu vaccine and antiviral medications (no date)
- News Releases
- FDA Approves Additional Vaccine for 2009 H1N1 Influenza Virus (November 16)
- FDA Expands Approved Use of H1N1 Vaccines to Include Infants and Children (November 12)
- FDA Commissioner Addresses Nation’s Healthcare Professionals on H1N1 Vaccine (November 10)
- FDA Approves Vaccines for 2009 H1N1 Influenza Virus (September 15)
- FDA Approves New Influenza Vaccine Production Facility (May 6)
Consumer Protection: Fraudulent H1N1 Claims and Bogus H1N1 Products
FDA tracks and prosecutes advertisers who make fraudulent claims in ads about preventing or treating the H1N1 virus.Antiviral Drugs
FDA ensures the safety, effectiveness and supply of flu antiviral drugs.- Drug Treatments for Flu (antivirals)
- Guidance to Pharmacies on Advance Compounding of Tamiflu Oral Suspension to Provide for Multiple Prescriptions (October 31)
- Updated Questions and Answers: 2009 H1N1 Flu Virus and Emergency Use Authorization of Tamiflu and Relenza (October 31)
- Peramivir IV Questions and Answers for Health Care Providers
- Q&A for Health Care Providers: Renal Dosing and Administration Recommendations for Peramivir IV (PDF, 22 KB)
- Pregnancy and antiviral use
- Tamiflu Oral Suspension Shortage Information
- Stockpiled Antivirals at or Nearing Expiration
- FDA public health alert: potential medication errors with Tamiflu for oral suspension (September 25)
- Information for healthcare professionals: authorization of use of expired Tamiflu for oral suspension (October 2)
- Dear health care professionals letter regarding 2009 H1N1 flu virus (June 18)
- FDA update on the H1N1 flu vaccine and antiviral medications (no date)
- Emergency use authorizations
- Emergency use authorizations questions and answers (April 28)
- FDA and CDC Information on Potential “Spot Shortages” of Supplies for Treating and Preventing Novel Influenza A (H1N1) (June 18)
- News Releases
Diagnostic Tests
FDA approves diagnostic tests for laboratories, clinics and doctor’s offices.- Medical devices for flu diagnosis and protection (October 16)
- Dear health care professionals letter regarding 2009 H1N1 flu virus (June 18)
- Health care professional fact sheet: interpreting swine influenza RT-PCR detection panel test results (May 2)
- Patient fact sheet: understanding swine flu kit test results (May 2009)
- Emergency Use Authorizations for Devices (April 28)
- News Releases
Safety of the Food Supply
FDA ensures the safety of the food supply.Back to Top
Safety of the Blood Supply
Back to TopSupply of Masks, Gloves and Other Personal Protective Equipment
FDA monitors the supply of facemasks, respirators and other personal protective equipment.- Personal protective equipment – facemasks, respirators, etc. general information
- Questions and answers
- FDA and personal protective equipment for the 2009 H1N1 flu virus (September 15)
 |  |
-
-


|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||















Appendix A Current regulations for testing and regulatory approval of Vaccines
EMEA
- Guideline on submission of marketing-authorisation applications for pandemic influenza vaccines through the centralised procedure (CPMP Adopted March 2004) (EMEA/CPMP/4986/03)
- Guideline on dossier structure and content for pandemic influenza vaccine marketing-authorisation application (CPMP Adopted December 2008) (EMEA/CPMP/4717/03)
- EMEA/PDCO standard paediatric investigation plan for non-adjuvanted or adjuvanted pandemic influenza vaccines during a pandemic (PDCO adopted June 2009) (EMEA/405779/2009)
- Guideline on influenza vaccines prepared from viruses with the potential to cause a pandemic and intended for use outside of the core dossier context (CHMP adopted January 2007) (EMEA/CHMP/VWP/263499/2006)
- Core SPC for pandemic influenza vaccines (CHMP Adopted July 2009) (EMEA/CHMP/VEG/193031/04)
Risk Management Plans for pandemic influenza vaccines
FDA
9/27/2007
5/31/2007
5/31/2007
CDC
Vaccine Safety & Availability
- Common Ingredients in U.S. Licensed Vaccines
- Vaccine Adverse Events
Report adverse events (side effects) related to the administration of U.S. licensed vaccines - Vaccine Safety & Availability
- Influenza Virus Vaccine Safety & Availability
- Vaccine Safety Questions and Answers
- Recommendations for the Use of Vaccines Manufactured with Bovine-Derived Materials
- Thimerosal in Vaccines
- FDA and CDC Issue Alert on Menactra Meningococcal Vaccine and Guillain Barre Syndrome
FDA Press Release, September 30, 2005 - MMWR - Guillain-Barr� Syndrome Among Recipients of Menactra Meningococcal Conjugate Vaccine
MMWR Weekly Report, Centers for Disease Control, October 20, 2006 - Institute of Medicine (IOM) - Immunization Safety Review: Vaccines and Autism

-
WHO
Production and availability of pandemic influenza A (H1N1) vaccines
:: Safety and approval of pandemic influenza A (H1N1) vaccines
:: Use of pandemic influenza A (H1N1) vaccines
:: Seasonal influenza vaccines
:: Safety and approval of pandemic influenza A (H1N1) vaccines
:: Use of pandemic influenza A (H1N1) vaccines
:: Seasonal influenza vaccines
Lancet
Plennevaux E, Sheldon E, Blatter M, et al. Immune response after a single vaccination against 2009 influenza A H1N1 in USA: a preliminary report of two randomized controlled phase 2 trials. Lancet 2010 Jan 2;375(9708):41-8 [Full text]
Vajo Z, Tamas F, Sinka L, et al. Safety and immunogenicity of a 2009 pandemic influenza A H1N1 vaccine when administered alone or simultaneously with seasonal influenza vaccine for the 2009-10 influenza season: a multicentre, randomized controlled trial. Lancet 2010 Jan 2;375(9708):49-55 [Full text]
Liang X-F, Wang H-Q, Wang J-Z, et al. Safety and immunogenicity of 2009 pandemic influenza A H1N1 vaccines in China: a multicentre, double-blind, randomized, placebo-controlled trial. Lancet 2010 Jan 2;375(9708):56-66 [Full text]
Kelly H, Barr I. Large trials confirm immunogenicity of H1N1 vaccines. (Editorial) Lancet 2010 Jan 2;375(9708):6-8 [Full text]
Pfeifer D, Alfonso C, Wood D. Defining the safety profile of pandemic influenza vaccines. (Editorial) Lancet 2010 Jan 2;375(9708):9-11 [Full text]
Appendix B Seasonal Influenza Vaccine 2009
WHO
- an A/Brisbane/59/2007 (H1N1)-like virus; *
- an A/Brisbane/10/2007 (H3N2)-like virus; **
- a B/Brisbane/60/2008-like virus.
**A/Brisbane/10/2007 and A/Uruguay/716/2007 (an A/Brisbane/10/2007-like virus) are current vaccine viruses.
The influenza vaccine composition to be used in the 2009-2010 influenza season in the U.S. is identical to that recommended by the World Health Organization on February 12, 2009.
Appendix C.
Government Orders and Pricing Based on news media and press release.
 News")
 Scientific & Medical Resources")
These are some of the news headlines used for data extraction
Le virus H1N1 voyage à une vitesse incroyable
UK Receives 100,000 Doses of H1N1 Vaccine, Expects Licensure in OctoberU.S. CDC to Host Public Online Forum for H1N1 Vaccination Issues http://www.thelancet.com/H1N1-flu/egmn/0c03b3cf
Australia: The Australian company CSL projects to sell $300 million of influenza vaccine in 2009. The Australian government paid $90 million for 21 million doses.
France: 94 million doses of Pandemic vaccine ordered at a price of Euro 1000 million or $1500 million
USA : 195 million doses, stockpile of Tamiflu and Relenza, maybe Peramivir? Total budget $4.5 billion for 2009.
UK 90 million doses ordered, £ 2.2 billion funding provided for R&D to tackle H1N1 Pandemic
Germany : Ordered stockpile of Relenza to cover 30% of its population
Japan : 53 million doses of vaccine, 13-17 million domestic, rest imported, antivirals stockpile > 1 billion.
China : 5% of its population covered = 65 million doses = 650 million
10 local companies making the vaccine like SinoVac. Sino vac to supply 10 million doses at the rate of 2 million doses per month, Huanlang to supply 13 million and Shanghai Biologicals 10 million doses?
Local vaccine to cost 30% less, ie priced at $10 instead of $ 15 international price.
India 4 million doses ordered from Sanofi Aventis at a price of $15 per dose to cover healthcare providers and essential staff. Three local companies Serum Institute of India, Pune; Bharat Biotech, Hyderabad and Pancea Biotech have recieved WHO seed stock to manufacture Pandemic H1N1 flu vaccine by traditional method. India has no tradition of seasonal flu vaccination and clinical testing in local population is required to prove safety and efficacy. Cipla and other companies have made copies of Tamiflu and Relenza for export and to supply to Indian Government.
Brazil 18 million doses of vaccine ordered from Sanofi Aventis at a cost of $270 million.
Based on the direct orders from OECD countries to cover 70% of the population, the market is in the range of $9.2 billion. However, some of these orders may be filled in 2010 winter.
Appendix D Industry Response to Influenza A (H1N1) Pandemic
www.medimmune.com
H1N1 Glaxo Smith Kline http://www.gsk.com/media/index.htm
Novartis http://www.novartis.com/newsroom/swine-flu/
![[Ways to produce a flu vaccine chart]](http://s.wsj.net/public/resources/images/NA-BC268A_VACCI_NS_20091124215328.gif)




H1N1
Flu vaccine production
Flu vaccine filling & packaging
Vaccine R&D
Fact sheets:
Novartis Vaccines and Diagnostics (57 KB)
Flu Cell Culture Manufacturing and the Novartis Proprietary Cell Line (160 KB)
MF59® Adjuvant (63 KB)
Pandemic Influenza (51 KB)
Seasonal Influenza (65 KB)
This Pandemic Influenza Web site provides information for the public, health-care professionals, and the media on pandemic influenza, vaccines, and links to more information.
| Timeline of events surrounding sanofi pasteur's public health efforts regarding A(H1N1) |
H1N1 Glaxo Smith Kline http://www.gsk.com/media/index.htm
- H1N1 press releases
- Flu vaccine development process(PDF 442Kb)
- FAQs
- In focus: More about pandemic (H1N1) flu 2009
- Egg vs cell-based vaccine production (PDF 14Kb)
- Multimedia (B-roll and images)
Novartis http://www.novartis.com/newsroom/swine-flu/
Related materials:
H1N1
Flu vaccine production
Flu vaccine filling & packaging
Vaccine R&D
Fact sheets:
Novartis Vaccines and Diagnostics (57 KB)
Flu Cell Culture Manufacturing and the Novartis Proprietary Cell Line (160 KB)
MF59® Adjuvant (63 KB)
Pandemic Influenza (51 KB)
Seasonal Influenza (65 KB)
Flu vaccine development process
Egg vs cell-based vaccine production
Egg vs cell-based vaccine production
Related Knols
 " Swine Flu " Review")
 & Pregnancy: Vaccination and Treatment")
Appendix E List of approved Influenza Vaccines USA/Europe
Pandemic influenza vaccines centrally authorised in the EU
http://www.emea.europa.eu/pdfs/human/pandemicinfluenza/60825909en.pdfCelvapan |
Click on the name of each medicine in the table below to review its European public assessment report (EPAR).
| Vaccines developed for pandemic influenza | |
| Mock-up vaccines | Pre-pandemic vaccines |
FDA Approved Influenza Vaccines
- AFLURIA
CSL Limited (Afluria) - Fluarix
GlaxoSmithKline Biologicals - FluLaval
ID Biomedical Corp. of Quebec - FluMist
MedImmune, LLC - Fluvirin
Novartis Vaccines and Diagnostics Ltd. - Fluzone
Sanofi Pasteur, Inc.
Injectable Vaccines 2009 H1N1
- Influenza A (H1N1) 2009 Monovalent Vaccine (CSL Limited)
- Influenza A (H1N1) 2009 Monovalent Vaccine (ID Biomedical Corporation of Quebec)
- Influenza A (H1N1) 2009 Monovalent Vaccine (Novartis Vaccines and Diagnostics Limited)
- Influenza A (H1N1) 2009 Monovalent Vaccine (Sanofi Pasteur, Inc.)
Intranasal Vaccine
Appendix F Marketed Brands of Influenza Vaccines by Novartis
| Agrippal Highly purified influenza vaccine for adults and children above six months; one of the best tolerated influenza vaccines Learn more Novartis flu vaccines | |
| | |
| Begrivac A preservative-free influenza vaccine for adults and children above six months that is proven by years of experience Learn more Novartis flu vaccines | |
| | |
| Optaflu Cell culture-based influenza vaccine for adults above 18 years of age Learn more Novartis flu vaccines | |
| | |
| Fluad Active influenza immunization for the elderly, especially for patients with chronic conditions like diabetes or cardiovascular or respiratory diseases Learn more Novartis flu vaccines | |
| | |
| Fluvirin Subunit influenza vaccine that is a leading product in the US and is approved for sale in more than 20 countries Learn more Novartis flu vaccines | |
Other companies ( Sanofi Aventis, Glaxo Smith Kline ) have not provided a comprehensive list of marketed Influenza Vaccine Brands at their web sites.
Références
- Influenza in the Asia-Pacific The Lancet Infectious Diseases View PDF
- Garcia-Garcia L, Valdespino-Gómez JL, Lazcano-Ponce E, Jimenez-Corona A, Higuera-Iglesias A, Cruz-Hervert P, Cano-Arellano B, Garcia-Anaya A, Ferreira-Guerrero E, Baez-Saldaña R, Ferreyra-Reyes L, Ponce-de-León-Rosale
s S, Alpuche-Aranda C, Rodriguez-López MH, Perez-Padilla R, Hernandez-Avila M. Partial protection of seasonal trivalent inactivated vaccine against novel pandemic influenza A/H1N1 2009: case-control study in Mexico City. BMJ. 2009 Oct 6;339:b3928. doi: 10.1136/bmj.b3928. PubMed PMID: 19808768; PubMed Central PMCID: PMC2758337. - De Jong MD, Sanders RW. .The future of influenza vaccines. BMJ 2009;339:b4014. Published 6 October 2009, doi:10.1136/bmj.b401
4. - Wutzler, P. Schmidt-Ott, R. Hoyer H. Sauerbrei, A. Prevalence of influenza A and B antibodies in pregnant women and their offspring J. Clin. Virology. 2009, 46, 161-164. View PDF
- Salomon, R. Webster RG. The Influenza Virus Enigma\ Cell, 2009, 136 (3), 402-410
- Daems, R. Guidice, GD. Rappuoli, R. Anticipating crisis: Towards a pandemic vaccination strategy through alignment of public health and industrial policy. Vaccine 2005, 23, 5732-5742. Doi:10.1016/j.vaccin
e.2005.10.011. - Poland, GA. Jacobson, RM. Targonski, PV. Avian and Pandemic Influenza: An overview. Vaccine 2007, 25, 3057-3061. Doi:10.1016/j.vaccin
e.2007.01.050. - Palache, B. New Vaccine approaches for seasonal and pandemic influenza. Vaccine 2008, 26, 6332-6236. Doi:10.1016/j.vaccin
e.2008.07.022. - Maggon, Krishan. Influenza ( 2009 H1N1 ) Treatment Market:Global Sales of Influenza Antivirals [Internet]. Version 39. Knol. 2009 Oct 6.
http://knol.google.com/k/krishan-maggon/ influenza-2009-h1n1- treatment-market/3fy 5eowy8suq3/83 - Maggon K. R&D paradigm shift and billion dollar biologics. In Gad SC. (Ed.). Handbook of Pharmaceutical Biotechnology. John Wiley & Sons, New York. 2007, pp 161-199. ISBN 978-0-471-21386-4.
- Maggon K. Monoclonal antibody "gold rush". Curr Med Chem. 2007;14(18):1978-87. Review. PubMed PMID: 17691940.
- Maggon K. Industrial R&D paradigm shift to vaccines. Biotechnol J. 2009 Apr;4(4):458-61. PubMed PMID: 19370719.
- Tsang, KH. Samsatli, NJ. Shah N. Modelling and planning optimization of a complex flu vaccine facility. Trans IChemE. Food and Byproducts Processing 2006, 84 (C2), 123-134.Doi:10.1205/
fbp.05001. - 6. Carrat, F. Flahault, A. The challenge of antigenic drift. Vaccine. 2007, 25, 6852-6862. Doi:10.1016/j.vaccin
e.2007.07.027. - Monto, AS. Ansaldi, A. Aspinall, R. McElhaney JE. Montano, LF. Nichol, KL. Barbera JP. Schmitt, J. Stephenson, I. Influenza control in the 21st century:optimizing protection of older adults. Vaccine. 2009, 27, 5043-5053. Doi:10.1016/j.vaccin
e.2009.06.032. - Garten, RJ Davis, CT, Russel, CA, Shu, B. Lindstrom, S. et al. Antigenic and genetic characteristics of Swine-origin A (H1N1) Influenza viruses circulating in humans. Science 2009, 325, 197-201.
- Simonsen L, Viboud C, Taylor RJ, Miller MA. The epidemiology of influenza and its control. In: Rappuoli R, Del Giudice G, eds. Influenza vaccines for the future (Birkhaüser Verlag, Basel) 2008: 65-93.
- Osterhouse, ADME. Pre or post -pandemic influenza vaccine? 2007. Vaccine, 25, 4983-4984. doi:10:1016/j.vaccin
e.2007.05.033. - Leifer I, Lange E, Reimann I, Blome S, Juanola S, Duran JP, Beer M. Modified live marker vaccine candidate CP7_E2alf provides early onset of protection against lethal challenge infection with classical swine fever virus after both intramuscular and oral immunization. Vaccine. 2009 Sep 2. [Epub ahead of print] PubMed PMID: 19732859.
- Price GE, Soboleski MR, Lo CY, Misplon JA, Pappas C, Houser KV, Tumpey TM, Epstein SL. Vaccination focusing immunity on conserved antigens protects mice and ferrets against virulent H1N1 and H5N1 influenza A viruses. Vaccine. 2009 Sep 1. [Epub ahead of print] PubMed PMID: 19729082.
- De Groot AS, Ardito M, McClaine EM, Moise L, Martin WD. Immunoinformatic comparison of T-cell epitopes contained in novel swine-origin influenza A (H1N1) virus with epitopes in 2008-2009 conventional influenza vaccine. Vaccine. 2009 Sep 25;27(42):5740-7. Epub 2009 Aug 4. PubMed PMID: 19660593.
- Leifer I, Lange E, Reimann I, Blome S, Juanola S, Duran JP, Beer M. Modified live marker vaccine candidate CP7_E2alf provides early onset of protection against lethal challenge infection with classical swine fever virus after both intramuscular and oral immunization. Vaccine. 2009 Sep 2. [Epub ahead of print] PubMed PMID: 19732859.
- De Villiers PJT. Steele AD. Hiemstrac LA. Rappaport R. Dunning AJ, Gruber WC. Forrest BD. and the LAIV Elderly Study Trial Network. Efficacy and safety of a live attenuated influenza vaccine in adults 60 years of age and older. Vaccine 2009 Sept 30 Epub doi:10.1016/j.vaccin
e.2009.09.092 Article in press, uncorrected proof. - 2009 H1N1 Influenza Shots and Pregnant Women: Questions and Answers for Patients
- H1N1 Trials Begin for Pregnant Women
- Asthma Information for Patients and Parents of Patients
- The H1N1 flu pandemic. What you need to know. Mayo Clin Womens Healthsource. 2009 Nov;13(11):4-5. PubMed PMID: 19794334.
- Maggon K, Barik S. New drugs and treatment for respiratory syncytial virus. Rev Med Virol. 2004 May-Jun;14(3):149-68
. Review. PubMed PMID: 15124232. - Maggon, Krishan. Global Vaccine Market Review 2008 (World Top Ten Vaccines):World Leading Companies & Top Selling Vaccines 2008 [Internet]. Version 60. Knol. 2009 Sep 14.
http://knol.google.com/k/krishan-maggon/ global-vaccine-marke t-review-2008-world/ 3fy5eowy8suq3/8 - Djelouat, Salim; Maggon, Krishan; bhagia, minoo; Lahaye, Patrick. Influenza ( 2009 H1N1 ) & Pregnancy: Vaccination and Treatment:Swine Flu, Influenza A, H1N1 v, Pregnancy, High Risk, WHO, CDC, EMEA, FDA, Vaccination, 3rd Trimester, Antiviral,Tamiflu, Relenza, Breastfeeding [Internet]. Version 67. Knol. 2009 Oct 2.
http://knol.google.com/k/salim-djelouat/ influenza-2009-h1n1- pregnancy/1yexqll01w r4o/205 - Maggon, Krishan; Djelouat, Salim; Lahaye, Patrick. Influenza ( 2009 H1N1 ) Scientific & Medical Resources:Swine Flu, Influenza A, 2009 H1N1 , Pandemic, Medical, Scientific, links, medical journals, sites, videos, RSS feeds, original research papers [Internet]. Version 22. Knol. 2009 Sep 19.
http://knol.google.com/k/krishan-maggon/ influenza-2009-h1n1- scientific-medical/3 fy5eowy8suq3/80 - Maggon, Krishan. Global Pharmaceutical Market Review & World Top Ten/Twenty Drugs 2008:World Best Selling Human Medicinal Brands 2008, Top Ten, Top Twenty, First Global Market Report [Internet]. Version 142. Knol. 2009 Sep 14.
http://knol.google.com/k/krishan-maggon/ global-pharmaceutica l-market-review/3fy5 eowy8suq3/6 - Djelouat, Salim; Lahaye, Patrick; Maggon, Krishan. Influenza ( 2009 H1N1 ) " Swine Flu " Review:Swine Flu, Influenza, 2009 H1N1, Pandemic, Review, Flu Alert, Flu Info, Flu Fact File, Flu Q&A, Flu FAQ, Flu Advisory, Guidelines, WHO, CDC, FDA, ECDC, EMEA,images, CDC Slides, CDC videos, spread, mutation, vaccines, antivirals [Internet]. Version 223. Knol. 2009 Sep 20.
http://knol.google.com/k/salim-djelouat/ influenza-2009-h1n1- swine-flu-review/1ye xqll01wr4o/106 - Shohat, Murry; Baskerville, Peter; MEES, Gust; Jenkins, Garry; Maggon, Krishan; Baum, Lyonel; Djelouat, Salim; Lahaye, Patrick. Influenza Times & Swine Flu ( H1N1 ) News:Significant Influenza A ( H1N1 )/ Swine Flu news as it occurs, supporting PLoS Currents [Internet]. Version 958. Knol. 2009 Oct 2.
http://knol.google.com/k/murry-shohat/in fluenza-times-swine- flu-h1n1-news/2srzof gvr8kjr/26 - Lay, M. Callejo, B. Chang, S. Hong, DK. Lewis, DB. et al. Cationic lipid/DNA complexes (JRVS 100) combined with influenza vaccine (FluZone) increases antibody response, cellular immunity and antigenically driftet protection. Vaccine 2009, 27, 3811-3820. Doi:10.1016/j.vaccin
e.2009.04.054. - Raymond James Third Annual Vaccines Seminar, Paris, France Wayne Pisano, President & CEO, Sanofi Pasteur and Didier Hoch, President Sanofi Pasteur MSD, participated in the vaccines seminar. * Download the presentation by Wayne Pisano * Download the presentation by Didier Hoch
- Collin N, de Radiguès X; World Health Organization H1N1 Vaccine Task Force. Vaccine production capacity for seasonal and pandemic (H1N1) 2009 influenza. Vaccine. 2009 Aug 20;27(38):5184-6. Epub 2009 Jun 27. PubMed PMID: 19563891.
- Arya SC, Agarwal N. Apropos "vaccines in a hurry". Vaccine. 2009 Aug 6;27(36):4875. Epub 2009 Jun 26. PubMed PMID: 19560429.
- Eichner M, Schwehm M, Duerr HP, Brockmann SO. The influenza pandemic preparedness planning tool InfluSim. BMC Infect Dis. 2007 Mar 13;7:17. PubMed PMID: 17355639; PubMed Central PMCID: PMC1832202.
- Duerr HP, Brockmann SO, Piechotowski I, Schwehm M, Eichner M. Influenza pandemic intervention planning using InfluSim: pharmaceutical and non- pharmaceutical interventions. BMC Infect Dis. 2007 Jul 13;7:76. PubMed PMID: 17629919; PubMed Central PMCID: PMC1939851.
- Collier R. Revised WHO pandemic scale requires higher incidence of disease for most alert levels. CMAJ. 2009 Jun 9;180(12):E95-6. PubMed PMID: 19506267; PubMed Central PMCID: PMC2691422.
- Kresse H. Rovini H. Influenza vaccine market dynamics. Nature Reviews Drug Discovery 8, 841-842 (November 2009) | doi:10.1038/nrd3026
- Schnitzler SU, Schnitzler P. An update on swine-origin influenza virus A/H1N1: a review. Virus Genes. 2009 Oct 7. [Epub ahead of print] PubMed PMID: 19809872.
- Centers for Disease Control and Prevention (CDC). Update on Influenza A (H1N1) 2009 Monovalent Vaccines. MMWR Morb Mortal Wkly Rep. 2009 Oct 9;58(39):1100-1. PubMed PMID: 19816398.
- The ANZIC Influenza Investigators. Critical Care Services and 2009 H1N1 Influenza in Australia and New Zealand. N Engl J Med. 2009 Oct 8. [Epub ahead of print] PubMed PMID: 19815860.
- Jain S, Kamimoto L, Bramley AM, Schmitz AM, Benoit SR, Louie J, Sugerman DE, Druckenmiller JK, Ritger KA, Chugh R, Jasuja S, Deutscher M, Chen S, Walker JD, Duchin JS, Lett S, Soliva S, Wells EV, Swerdlow D, Uyeki TM, Fiore AE, Olsen SJ, Fry AM, Bridges CB, Finelli L; the 2009 Pandemic Influenza A (H1N1) Virus Hospitalizations Investigation Team. Hospitalized Patients with 2009 H1N1 Influenza in the United States, April-June 2009. N Engl J Med. 2009 Oct 8. [Epub ahead of print] PubMed PMID: 19815859.
- Rehm SJ, Farley MM, File TM Jr, Hall WJ, Hopkins R, Levine OS, Nichol KL, Nuorti P, Zimmerman RK, Schaffner W. Higher Pneumococcal Disease Vaccination Rates Needed to Protect More At-Risk US Adults. Postgrad Med. 2009 Nov;121(6):101-5. PubMed PMID: 19940420.
- Ofri D. The Emotional Epidemiology of H1N1 Influenza Vaccination. N Engl J Med. 2009 Nov 25. [Epub ahead of print] PubMed PMID: 19940291.
- Chowell, Gerardo; Viboud, Cecile; Wang, Xiaohong; Bertozzi, Stefano; Miller, Mark. Adaptive vaccination strategies to mitigate pandemic influenza:Mexico as a case study [Internet]. Version 34. PLoS Currents: Influenza. 2009 Aug 17 [revised 2009 Aug 18]:RRN1004.
http://knol.google.com/k/gerardo-chowell /adaptive-vaccinatio n-strategies-to/35hp bywfdwl4n/3 - Irvine DV, Goto DB, Vaughn MW, Nakaseko Y, McCombie WR, Yanagida M, Martienssen R. Mapping epigenetic mutations in fission yeast using whole-genome next-generation sequencing. Genome Res. 2009 Jun;19(6):1077-83. Epub 2009 May 7. PubMed PMID: 19423874; PubMed Central PMCID: PMC2694473.
- Nuño M, Chowell G, Gumel AB. Assessing the role of basic control measures, antivirals and vaccine in curtailing pandemic influenza: scenarios for the US, UK and the Netherlands. J R Soc Interface. 2007 Jun 22;4(14):505-21. PubMed PMID: 17251132; PubMed Central PMCID: PMC2373400.
- Mylius SD, Hagenaars TJ, Lugnér AK, Wallinga J. Optimal allocation of pandemic influenza vaccine depends on age, risk and timing. Vaccine. 2008 Jul 4;26(29-30):3742-9. Epub 2008 May 7. PubMed PMID: 18524428.
- MacDonald N. H1N1 influenza vaccine: Global access for a global problem. CMAJ. 2009 Aug 4;181(3-4):123, E30-1. Epub 2009 Jun 18. English, French. PubMed PMID: 19541727; PubMed Central PMCID: PMC2717664.
- Chowell G, Bertozzi SM, Colchero MA, Lopez-Gatell H, Alpuche-Aranda C, Hernandez M, Miller MA. Severe respiratory disease concurrent with the circulation of H1N1 influenza. N Engl J Med. 2009 Aug 13;361(7):674-9. Epub 2009 Jun 29. PubMed PMID: 19564633.
- Zimmer SM, Burke DS. Historical perspective--Emergen
ce of influenza A (H1N1) viruses. N Engl J Med. 2009 Jul 16;361(3):279-85. Epub 2009 Jun 29. PubMed PMID: 19564632. - Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, Ramirez-Venegas A, Rojas-Serrano J, Ormsby CE, Corrales A, Higuera A, Mondragon E, Cordova-Villalobos JA; INER Working Group on Influenza. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009 Aug 13;361(7):680-9. Epub 2009 Jun 29. PubMed PMID: 19564631.
- Morens DM, Taubenberger JK, Fauci AS. The persistent legacy of the 1918 influenza virus. N Engl J Med. 2009 Jul 16;361(3):225-9. Epub 2009 Jun 29. Erratum in: N Engl J Med. 2009 Sep 10;361(11):1123. PubMed PMID: 19564629; PubMed Central PMCID: PMC2749954.
- Tran TH, Ruiz-Palacios GM, Hayden FG, Farrar J. Patient-oriented pandemic influenza research. Lancet. 2009 Jun 20;373(9681):2085-6. PubMed PMID: 19541022.
- Price LC. Should I have an H1N1 flu vaccination after Guillain-Barre syndrome? BMJ. 2009 Sep 9;339:b3577. doi: 10.1136/bmj.b3577. PubMed PMID: 19740925.
- Erlewyn-Lajeunesse M, Brathwaite N, Lucas JS, Warner JO. Recommendations for the administration of influenza vaccine in children allergic to egg. BMJ. 2009 Sep 15;339:b3680. doi: 10.1136/bmj.b3680. Review. PubMed PMID: 19755545.
- Hancock K, Veguilla V, Lu X, Zhong W, Butler EN, Sun H, Liu F, Dong L, Devos JR, Gargiullo PM, Brammer TL, Cox NJ, Tumpey TM, Katz JM. Cross-Reactive Antibody Responses to the 2009 Pandemic H1N1 Influenza Virus. N Engl J Med. 2009 Sep 10. [Epub ahead of print] PubMed PMID: 19745214.
- Clark TW, Pareek M, Hoschler K, Dillon H, Nicholson KG, Groth N, Stephenson I. Trial of Influenza A (H1N1) 2009 Monovalent MF59-Adjuvanted Vaccine -- Preliminary Report. N Engl J Med. 2009 Sep 10. [Epub ahead of print] PubMed PMID: 19745215.
- Greenberg ME, Lai MH, Hartel GF, Wichems CH, Gittleson C, Bennet J, Dawson G, Hu W, Leggio C, Washington D, Basser RL. Response after One Dose of a Monovalent Influenza A (H1N1) 2009 Vaccine -- Preliminary Report. N Engl J Med. 2009 Sep 10. [Epub ahead of print] PubMed PMID: 19745216.
- Lister P, Reynolds F, Parslow R, Chan A, Cooper M, Plunkett A, Riphagen S, Peters M. Swine-origin influenza virus H1N1, seasonal influenza virus, and critical illness in children. Lancet. 2009 Aug 22;374(9690):605-7. PubMed PMID: 19700000.
- Verheyen J, Balduin M, Kaiser R, Pfister H. Seasonal influenza species in people analysed for the presence of the pandemic (H1N1) 2009 influenza virus. J Clin Microbiol. 2009 Sep 30. [Epub ahead of print] PubMed PMID: 19794039.
- Peiris JS, Tu WW, Yen HL. A novel H1N1 virus causes the first pandemic of the 21(st) Century. Eur J Immunol. 2009 Sep 29. [Epub ahead of print] PubMed PMID: 19790188.
- Kieny MP. WHO supports fair access to influenza A (H1N1) vaccine. Bull World Health Organ. 2009 Sep;87(9):653-4. PubMed PMID: 19784443; PubMed Central PMCID: PMC2739921.
- Wiwanitkit V. Finding a new drug and vaccine for emerging swine flu: What is the concept? Biologics. 2009;3:377-83. Epub 2009 Sep 15. PubMed PMID: 19774205; PubMed Central PMCID: PMC2747336.
- Sylte MJ, Suarez DL. Influenza neuraminidase as a vaccine antigen. Curr Top Microbiol Immunol. 2009;333:227-41. PubMed PMID: 19768409.
- Fiore AE, Bridges CB, Cox NJ. Seasonal influenza vaccines. Curr Top Microbiol Immunol. 2009;333:43-82. PubMed PMID: 19768400.
- Michaelis M, Doerr HW, Cinatl J Jr. An Influenza A H1N1 Virus Revival - Pandemic H1N1/09 Virus. Infection. 2009 Sep 18. [Epub ahead of print] PubMed PMID: 19768379.
- Arya SC, Nirmala A. Influenza A (H1N1) 2009 monovalent vaccine: Laboratory confirmation of vaccine breakdowns. Vaccine. 2009 Sep 16. [Epub ahead of print] PubMed PMID: 19765396.
- Kuehn BM. CDC names H1N1 vaccine priority groups. JAMA. 2009 Sep 16;302(11):1157-8. PubMed PMID: 19755687.
- Salles MJ, Sens YA, Boas LS, Machado CM. Influenza virus vaccination in kidney transplant recipients: serum antibody response to different immunosuppressive drugs. Clin Transplant. 2009 Sep 14. [Epub ahead of print] PubMed PMID: 19758368.
- Yamada T. Poverty, wealth, and access to pandemic influenza vaccines. N Engl J Med. 2009 Sep 17;361(12):1129-31. Epub 2009 Aug 12. PubMed PMID: 19675324.
- Lipsitch M, Riley S, Cauchemez S, Ghani AC, Ferguson NM. Managing and reducing uncertainty in an emerging influenza pandemic. N Engl J Med. 2009 Jul 9;361(2):112-5. Epub 2009 May 27. PubMed PMID: 19474417.
- Baden LR, Drazen JM, Kritek PA, Curfman GD, Morrissey S, Campion EW. H1N1 influenza A disease--information for health professionals. N Engl J Med. 2009 Jun 18;360(25):2666-7. Epub 2009 May 7. PubMed PMID: 19423873.
- Shinde V, Bridges CB, Uyeki TM, Shu B, Balish A, Xu X, Lindstrom S, Gubareva LV, Deyde V, Garten RJ, Harris M, Gerber S, Vagasky S, Smith F, Pascoe N, Martin K, Dufficy D, Ritger K, Conover C, Quinlisk P, Klimov A, Bresee JS, Finelli L. Triple-reassortant swine influenza A (H1) in humans in the United States, 2005-2009. N Engl J Med. 2009 Jun 18;360(25):2616-25. Epub 2009 May 7. Erratum in: N Engl J Med. 2009 Jul 2;361(1):102. PubMed PMID: 19423871.
- Novel Swine-Origin Influenza A (H1N1) Virus Investigation Team, Dawood FS, Jain S, Finelli L, Shaw MW, Lindstrom S, Garten RJ, Gubareva LV, Xu X, Bridges CB, Uyeki TM. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. N Engl J Med. 2009 Jun 18;360(25):2605-15. Epub 2009 May 7. Erratum in: N Engl J Med. 2009 Jul 2;361(1):102. PubMed PMID: 19423869.
- Brownstein JS, Freifeld CC, Madoff LC. Influenza A (H1N1) virus, 2009--online monitoring. N Engl J Med. 2009 May 21;360(21):2156. Epub 2009 May 7. PubMed PMID: 19423868.
- Lipsitch M, Hayden FG, Cowling BJ, Leung GM. How to maintain surveillance for novel influenza A H1N1 when there are too many cases to count. Lancet. 2009 Aug 11. [Epub ahead of print] PubMed PMID: 19679345.
- Mangtani P, Mak TK, Pfeifer D. Pandemic H1N1 infection in pregnant women in the USA. Lancet. 2009 Aug 8;374(9688):429-30. PubMed PMID: 19665629.
- Jamieson DJ, Honein MA, Rasmussen SA, Williams JL, Swerdlow DL, Biggerstaff MS, Lindstrom S, Louie JK, Christ CM, Bohm SR, Fonseca VP, Ritger KA, Kuhles DJ, Eggers P, Bruce H, Davidson HA, Lutterloh E, Harris ML, Burke C, Cocoros N, Finelli L, MacFarlane KF, Shu B, Olsen SJ; Novel Influenza A (H1N1) Pregnancy Working Group. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet. 2009 Aug 8;374(9688):451-8. Epub 2009 Jul 28. PubMed PMID: 19643469.
- Daems, R. Guidice, GD. Rappuoli, R. Anticipating crisis: Towards a pandemic vaccination strategy through alignment of public health and industrial policy. Vaccine 2005, 23, 5732-5742. Doi:10.1016/j.vaccin
e.2005.10.011. - The CDC’s Recommendations for Influenza A (H1N1) 2009 Vaccine
- Tamma PD, Ault KA, Del Rio C, Steinhoff MC, Halsey NA, Omer SB. Safety of influenza vaccination during pregnancy. Am J Obstet Gynecol. 2009 Oct 20. [Epub ahead of print] PubMed PMID: 19850275.
- Eisen DP, McBryde ES. Avoiding Guillan-Barré Syndrome following swine origin pandemic H1N1 2009 influenza vaccination. J Infect Dis. 2009 Nov 15;200(10):1627-8. PubMed PMID: 19857155.
- Zhu FC, Wang H, Fang HH, Yang JG, Lin XJ, Liang XF, Zhang XF, Pan HX, Meng FY, Hu YM, Liu WD, Li CG, Li W, Zhang X, Hu JM, Peng WB, Yang BP, Xi P, Wang HQ, Zheng JS. A Novel Influenza A (H1N1) Vaccine in Various Age Groups. N Engl J Med. 2009 Oct 21. [Epub ahead of print] PubMed PMID: 19846844.
- Kramarz P, Ciancio B, Nicoll A. Seasonal and pandemic influenza vaccines for the elderly and other risk groups: a review of available data. Pol Arch Med Wewn. 2009 Oct;119(10):654-9. PubMed PMID: 19847142.
- Louie JK, Acosta M, Winter K, Jean C, Gavali S, Schechter R, Vugia D, Harriman K, Matyas B, Glaser CA, Samuel MC, Rosenberg J, Talarico J, Hatch D; for the California Pandemic (H1N1) Working Group. Factors Associated With Death or Hospitalization Due to Pandemic 2009 Influenza A(H1N1) Infection in California. JAMA. 2009 Nov 4;302(17):1896-1902. PubMed PMID: 19887665.
- Black S, Eskola J, Siegrist CA, Halsey N, Macdonald N, Law B, Miller E, Andrews N, Stowe J, Salmon D, Vannice K, Izurieta HS, Akhtar A, Gold M, Oselka G, Zuber P, Pfeifer D, Vellozzi C. Importance of background rates of disease in assessment of vaccine safety during mass immunisation with pandemic H1N1 influenza vaccines. Lancet. 2009 Oct 30. [Epub ahead of print] PubMed PMID: 19880172.
- Wanitchang A, Kramyu J, Jongkaewwattana A. Enhancement of Reverse Genetics-derived Swine-Origin H1N1 Influenza Virus Seed Vaccine Growth by Inclusion of Indigenous Polymerase PB1 Protein. Virus Res. 2009 Oct 29. [Epub ahead of print] PubMed PMID: 19879908.
- Davies J. Swine flu vaccines: reaching the finish line. Cell. 2009 Oct 30;139(3):449-51. PubMed PMID: 19879829.
- Bodewes R, Kreijtz JH, Rimmelzwaan GF. Yearly influenza vaccinations: a double-edged sword? Lancet Infect Dis. 2009 Oct 29. [Epub ahead of print] PubMed PMID: 19879807.
- Breitstein, J. Vaccines for All. Pharmaceut. Exec. 2009, 29, 40-52.
- Bansal, Shweta; Pourbohloul, Babak; Grenfell, Bryan; Meyers, Lauren Ancel. The Shifting Demographic Landscape of Influenza [Internet]. Version 40. PLoS Currents: Influenza. 2009 Sep 30 [revised 2009 Oct 1]:RRN1047.
http://knol.google.com/k/shweta-bansal/t he-shifting-demograp hic-landscape-of/tkw n3sjme3vo/1 - Presanis, Anne M; Lipsitch, Marc; Daniela De Angelis; New York City Department of Health and Mental Hygiene, Swine Flu Investigation Team,; Hagy, Angie; Reed, Carrie; Riley, Steven; Cooper, Ben; Biedrzycki, Paul; Finelli, Lyn. The severity of pandemic H1N1 influenza in the United States, April – July 2009 [Internet]. Version 23. PLoS Currents: Influenza. 2009 Sep 25 [revised 2009 Oct 2]:RRN1042.
http://knol.google.com/k/anne-m-presanis /the-severity-of-pan demic-h1n1-influenza /agr0htar1u6r/16 - Caplan AL. Unlicensed pandemic influenza A H1N1 vaccines. Lancet. 2009 Nov 13. [Epub ahead of print] PubMed PMID: 19914708.
- Centers for Disease Control and Prevention (CDC). Effectiveness of 2008-09 trivalent influenza vaccine against 2009 pandemic influenza A (H1N1) - United States, May-June 2009. MMWR Morb Mortal Wkly Rep. 2009 Nov 13;58(44):1241-5. PubMed PMID: 19910912.
- Mahlmeister LR. Best practices in perinatal care: prevention and treatment of novel influenza A (H1N1) virus during pregnancy and the immediate postbirth period. J Perinat Neonatal Nurs. 2009 Oct-Dec;23(4):307-11
. PubMed PMID: 19915412. - Beigi RH, Wiringa AE, Bailey RR, Assi TM, Lee BY. Economic Value of Seasonal and Pandemic Influenza Vaccination during Pregnancy. Clin Infect Dis. 2009 Nov 13. [Epub ahead of print] PubMed PMID: 19911967.
- Swine flu--hard to keep up with new developments. Child Health Alert. 2009 Oct;27:1-2. PubMed PMID: 19916184.
- Jain R, Goldman RD. Novel influenza A(H1N1): clinical presentation, diagnosis, and management. Pediatr Emerg Care. 2009 Nov;25(11):791-6. PubMed PMID: 19915434.
- Echevarría-Zuno S, Mejía-Aranguré JM, Mar-Obeso AJ, Grajales-Muñiz C, Robles-Pérez E, González-León M, Ortega-Alvarez MC, Gonzalez-Bonilla C, Rascón-Pacheco RA, Borja-Aburto VH. Infection and death from influenza A H1N1 virus in Mexico: a retrospective analysis. Lancet. 2009 Nov 11. [Epub ahead of print] PubMed PMID: 19913290.
- Koudstaal W, Koldijk MH, Brakenhoff JP, Cornelissen LA, Weverling GJ, Friesen RH, Goudsmit J. Pre- and Postexposure Use of Human Monoclonal Antibody against H5N1 and H1N1 Influenza Virus in Mice: Viable Alternative to Oseltamivir. J Infect Dis. 2009 Nov 13. [Epub ahead of print] PubMed PMID: 19911992.
- Nishiura H, Iwata K. A simple mathematical approach to deciding the dosage of vaccine against pandemic H1N1 influenza. Euro Surveill. 2009 Nov 12;14(45). pii: 19396. PubMed PMID: 19941790.
- Tsai T, Kyaw MH, Novicki D, Nacci P, Rai S, Clemens R. Exposure to MF59-adjuvanted influenza vaccines during pregnancy-A retrospective analysis. Vaccine. 2009 Dec 4. [Epub ahead of print] PubMed PMID: 19969117.
- Chan PK. Lancet conference: influenza in the Asia-Pacific and the international scientific symposium on influenza pandemic response and preparedness. Expert Rev Anti Infect Ther. 2009 Dec;7(10):1165-6. PubMed PMID: 19968508.
- Martin V. Coding for the H1N1 virus vaccination. Med Econ. 2009 Oct 23;86(20):26. PubMed PMID: 19967852.
- Greene SK, Kulldorff M, Lewis EM, Li R, Yin R, Weintraub ES, Fireman BH, Lieu TA, Nordin JD, Glanz JM, Baxter R, Jacobsen SJ, Broder KR, Lee GM. Near Real-Time Surveillance for Influenza Vaccine Safety: Proof-of-Concept in the Vaccine Safety Datalink Project. Am J Epidemiol. 2009 Dec 4. [Epub ahead of print] PubMed PMID: 19965887.
- Greene SK, Kulldorff M, Lewis EM, Li R, Yin R, Weintraub ES, Fireman BH, Lieu TA, Nordin JD, Glanz JM, Baxter R, Jacobsen SJ, Broder KR, Lee GM. Near Real-Time Surveillance for Influenza Vaccine Safety: Proof-of-Concept in the Vaccine Safety Datalink Project. Am J Epidemiol. 2009 Dec 4. [Epub ahead of print] PubMed PMID: 19965887.
- Pascua PN, Song MS, Lee JH, Park KJ, Kwon HI, Baek YH, Hong SP, Rho JB, Kim CJ, Poo H, Ryoo TS, Sung MH, Choi YK. Evaluation of the efficacy and cross-protectivity of recent human and swine vaccines against the pandemic (H1N1) 2009 virus infection. PLoS One. 2009 Dec 23;4(12):e8431. PubMed PMID: 20037716.
- Roman F, Vaman T, Gerlach B, Markendorf A, Gillard P, Devaster JM. Immunogenicity and safety in adults of one dose of influenza A H1N1v 2009 vaccine formulated with and without AS03(A)-adjuvant: Preliminary report of an observer-blind, randomized trial. Vaccine. 2009 Dec 21. [Epub ahead of print] PubMed PMID: 20034605.
- De Groot AS, Ardito M, McClaine EM, Moise L, Martin WD. Immunoinformatic comparison of T-cell epitopes contained in novel swine-origin influenza A (H1N1) virus with epitopes in 2008-2009 conventional influenza vaccine. Vaccine. 2009 Sep 25;27(42):5740-7. Epub 2009 Aug 4. PubMed PMID: 19660593.
Aucun commentaire:
Enregistrer un commentaire